“History is about storytelling, while medicine, at its core, is a storytelling discipline as well,” said Matthew Klingle, when asked to consider what a professional historian brings to the study of medical science.

Klingle is associate professor of history and environmental studies, and for the past decade or so he has been immersed in the study of public health and chronic disease, particularly diabetes.
“Even if you take medicine as science in its most reductive sense—in the laboratory with vials and microscopes and slides and samples—eventually that research is going to be translated into a physician talking to a patient who is in pain and who is worried,” he said. “That physician is then going to have to administer a diagnosis that relies upon both the rigor of science and the empathy of a compassionate listener who can process that person’s story and find a way to alleviate the suffering.” In this sense, explained Klingle, medicine is the ultimate “humanities” subject, relying as it does on communication between individuals and understanding how the past can affect the present.
Klingle’s current book project, tentatively titled Sweet Blood: Diabetes and the Changing Nature of Modern Health (currently under contract with Yale University Press), explores how environmental and cultural factors have shaped the history of the disease from the nineteenth century to the present day.
There are two main types of diabetes, both of them characterized by high blood sugar levels. The most common—affecting 90 to 95 percent of sufferers—is known as type 2 diabetes, where the body fails to produce enough insulin (a hormone made by the pancreas that regulates our intake of glucose, the main sugar found in blood) or to use insulin properly. Type 1 diabetes is due to the loss of beta cells in the pancreas, which as a result fails to produce enough insulin to regulate blood sugar levels.
In addition to the measurable factors that can contribute to a person’s likelihood of developing the disease—poor nutrition, obesity, exposure to certain toxic substances—Klingle also aims to highlight the less quantifiable factors. The simple truth, he explained, is that your exposure to a chronic disease like diabetes is inextricably tied up with what socioeconomic class you’re from and what race you are. Diabetes disproportionately affects poor communities and especially communities of color, said Klingle. “Health is a function of access, wealth, and privilege. For a long time, certain communities, certain bodies, were not seen as being normal or healthy or deserving of greater understanding.”
For example, he explained, African Americans have traditionally been regarded as innately predisposed to conditions like diabetes, kidney failure, and hypertension. “Until recently, some medical schools taught that African American bodies are different from white bodies. But what medicine is asking now, thanks in part to the work of social science and humanities scholars, is ‘To what degree are these differences with Black bodies something that we've built up as a construct over time?’” Race and inequality are social phenomena, but these social facts lead to more than discrimination in health care. They can also leave lasting physiological damage. In other words, added Klingle, there’s a strong argument linking structural inequalities with ill health.
“I think about history as less of an assemblage of facts and information and more of a way of thinking that reminds us that we live in a complicated world, compelling us to act with both humanity and humility."
Klingle’s book project recently received a boost in the form of $100,000 in grant money from the National Library of Medicine of the National Institutes of Health, payable over two years in $50,000 disbursements. The award (grant number 1G13LM014433-01) enables Klingle to take sabbatical leave and focus on completing a full draft of the book, submitting the final manuscript to the publisher in the summer of 2025.
It's not just journals and textbooks Klingle is poring over, but rare manuscripts, interviews, and personal accounts in order to provide context and perspective to the subject. “This book is aimed at the general, informed reader, as well as medical professionals,” he explained, “and I aim to use examples of individual stories and anecdotes as a way of personalizing big issues.”
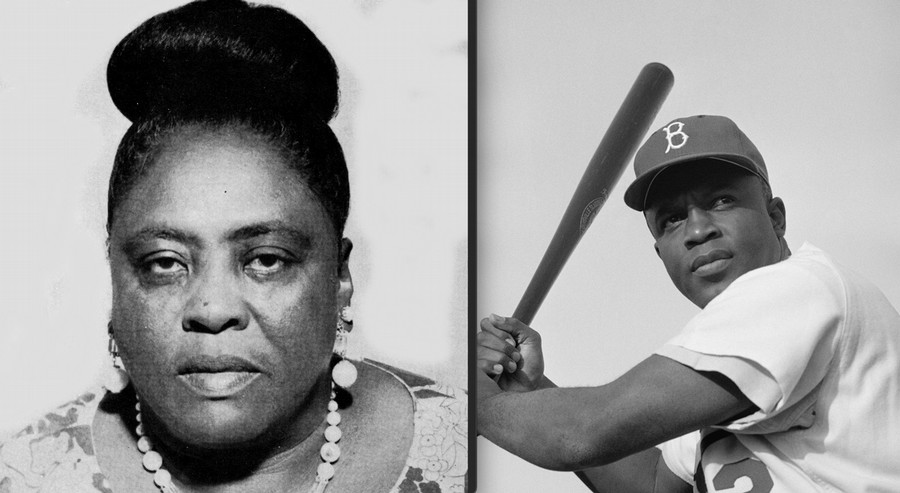
For example, in a chapter examining links between stress and chronic illness, Klingle looks at baseball legend Jackie Robinson, whose early death at fifty-three was due to diabetes-related heart problems. He also highlights the civil rights activists Fannie Lou Hamer, who died in her fifties after suffering years of health problems, including diabetes. (It was Hamer who famously said she was “sick and tired of being sick and tired.”) Klingle wants people to consider the extent to which the stress of racial discrimination was to blame for the health problems of people like Robinson and Hamer.
Chronic diseases like diabetes can have many causes, said Klingle, and it’s often hard to say exactly how much factors like exercise, lifestyle, environmental exposure, and sociological inequalities are to blame. “One thing’s for sure, however,” he stressed. “Our bodies keep the score. They act as a kind of archive of all the benefits we've had in our lives as well as the assaults, and those things can be cumulatively measured across populations.”
Historians, he said, have a key role to play in making sense of big issues like public health.
“I think about history as less of an assemblage of facts and information and more of a way of thinking that reminds us that we live in a complicated world, compelling us to act with both humanity and humility. It all comes back again to the important role humanities scholars contribute to a subject like medicine because of the perspective they bring.”
“Sure, medicine is about machines that go ‘ping’ and data and pharmacology,” said Klingle, “but it’s also about fear, hope, joy, sorrow, grief, all those things that are in the realm of the humanities. Seeing medicine as humanities can be a reminder that while we are all, ultimately, flesh and bones, we do not possess the same flesh and the same bones. And history is the reason why.”